Treatment of Lyme disease
The first-line treatment for Lyme disease in adults is doxycycline, a tetracycline antibiotic. Other effective antibiotics include amoxicillin (a penicillin-like antibiotic) and cefuroxime (Ceftin), a second generation cephalosporin. Most cases are treated with oral antibiotics, but intravenous antibiotics may be indicated for more complex cases such as neurologic-Lyme disease with meningitis, or certain cases of late Lyme arthritis.
Antimicrobials are critical for treating Lyme disease because without them, Borrelia burgdorferi, can evade the immune system, disseminate through the bloodstream, and persist in the body. Antibiotics work by either stopping the bacterial multiplication (doxycycline) or disrupting the cell wall to kill the bacteria (penicillins). By halting bacterial growth or killing the bacteria directly, antibiotics enable the immune system to eradicate the residual infection more effectively.
Side effects and Management
Like all medications, antibiotics can cause side effects. Patients should contact their healthcare provider if an itchy red rash develops while taking antibiotics.
Herxheimer Reaction: Some patients experience worsening symptoms during the first few days of treatment. This temporary reaction occurs when dying bacteria release products that stimulate the immune system to produce inflammatory cytokines and chemokines, causing increased fever and body aches. This should resolve within 24 to 48 hours after starting antibiotics.
Gastrointestinal Effects: The most common side effect of penicillin antibiotics is diarrhea. In rare cases, antibiotic use can lead to Clostridium difficile overgrowth, a serious condition that occurs when antibiotics kill beneficial gut bacteria. Probiotics may help restore healthy gut bacteria and microbiome balance.
Prognosis with Early Treatment
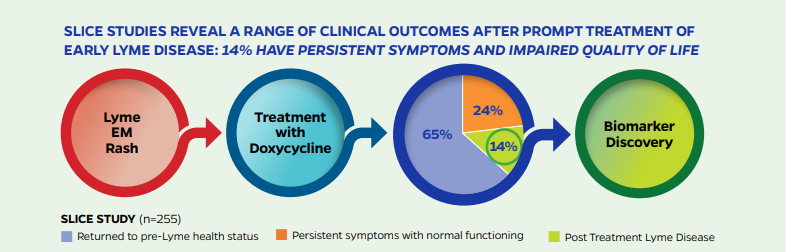
The prognosis after early treatment of Lyme disease is generally very good, and most patients recover fully after antibiotic treatment and return to their normal state of health. However, the prognosis worsens significantly when diagnosis and treatment are delayed.
Post-Treatment Lyme Disease (PTLD)
Research studies show that 14-20% of patients continue to experience debilitating ongoing or recurrent symptoms after appropriate antibiotic treatment for Lyme disease.
A rigorously designed prospective controlled research study published by the Johns Hopkins Lyme Disease Research Center and Clinical Care Program in 2022 found that even in a best case scenario when Lyme disease patients were diagnosed early and treated promptly with 21 days of doxycycline, 14% developed Post Treatment Lyme Disease (PTLD). compared with 4% in a healthy control group. In real-world settings with misdiagnoses and treatment delays, the risk for PTLD is likely even higher.
What is Post Treatment Lyme Disease?
Post Treatment Lyme Disease (PTLD) is a defined research subset of patients who remain significantly ill 6 months or more following standard antibiotic therapy for Lyme disease. PTLD is characterized by severe fatigue, musculoskeletal pain, sleep disturbance, depression, and cognitive problems such as difficulty with short-term memory, processing speed, or multi-tasking. Although often invisible to others, PTLD symptoms are debilitating and significantly impact patients’ health, quality of life, and daily functioning.
Our research demonstrates that the chronic symptom burden related to PTLD is substantial and statistically significantly greater than the normal aches and pains experienced by healthy individuals.
Symptoms of PTLD
- Severe fatigue
- Musculoskeletal pain
- Sleep disturbance
- Depression
- Cognitive impairment (memory, focus, processing speed, multitasking)
- Headaches
- Neck pain
- Temperature sensitivity
- Heart palpitations
- Other neurologic symptoms
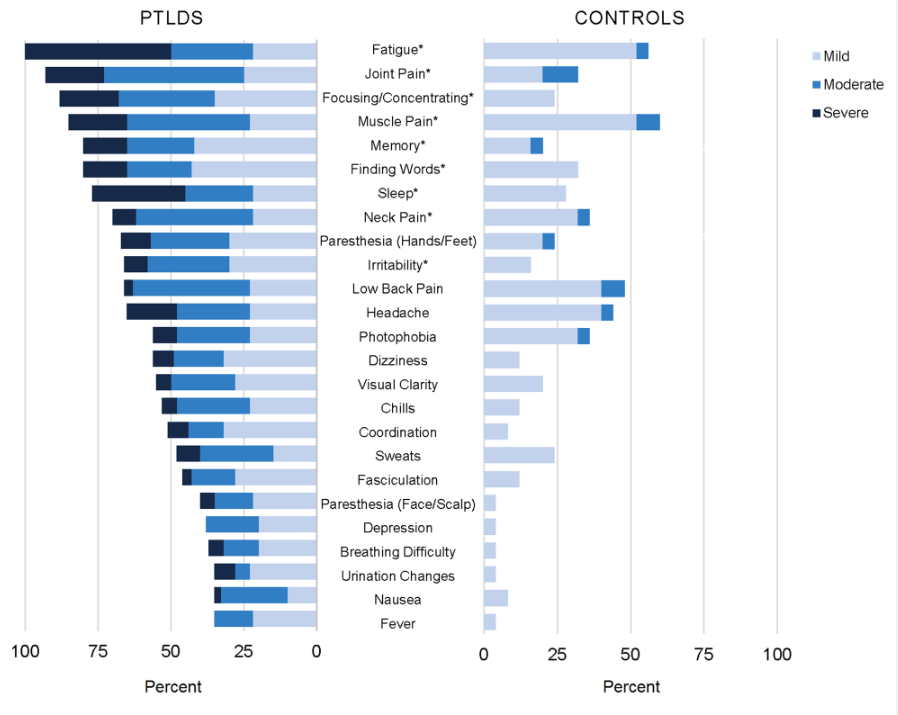
The chronic symptom burden related to Lyme disease is considerable, as shown on the left side of the graph above, and statistically significantly greater severity than the aches and pains of daily living experienced by the control group, on the right.
Risk Factors for Post Treatment Lyme Disease
Several factors increase the risk of developing Post Treatment Lyme Disease:
- Delay in diagnosis: Later treatment initiation increases PTLD risk
- Severity of initial illness: More severe initial symptoms correlate with higher risk
- Neurologic involvement: PTLD rates may be as high as 20% or higher in patients with neurologic Lyme disease
- Initial misdiagnosis: Incorrect initial diagnosis delays appropriate treatment
Additional risk factors under investigation include genetic predispositions, immunologic variables, and co-infections with other infections, such as tick-borne pathogens, that may contribute to more prolonged and complicated illness.
What causes Post Treatment Lyme Disease?
The causes of PTLD are not yet fully understood but are likely multifactorial. Our Center is investigating several potential mechanisms, including:
- Infection-induced immune dysfunction or auto-immunity
- Chronic inflammation
- Persistent bacterial infection or bacterial debris
- Neural network alteration
- Other tick-borne infections
- Other biologic mechanisms
The term PTLD does not assume any single underlying mechanism. The Lyme disease patient population is heterogeneous, and the drivers of persistent illness can be varied.
PTLD is a narrow research definition designed to facilitate systematic investigation, but findings can be extrapolated when appropriate to the broader population of patients with chronic or persistent Lyme disease symptoms.
Current Treatment Options
Currently, there are no FDA-approved treatments specifically for Post Treatment Lyme Disease. Therefore, treatment must be individualized to address each patient’s specific symptoms, findings, and circumstances.
To advance evidence-based care, our Center is conducting pilot clinical trials to evaluate new treatment approaches, made possible by the generous support of the Steven and Alexandra Cohen Foundation and the Clinical Trials Network.
Supporting Recovery and Well-being
While research continues into targeted treatments for Lyme infection associated chronic illness, may patients benefit from supportive care strategies that address overall health and symptom managment.
The following evidence-based lifestyle approaches can help support the body’s healing processes and improve quality of life:
Sleep
- Aim for 8 hours of quality sleep at consistent times each night
Physical Activity
- Regular exercise, aiming for 30 minutes per day if able (adjust based on individual tolerance)
Nutrition
- A balanced, nutrient-rich diet, ideally organic, including 4-9 servings of fruits and vegetables and 8 glasses of water daily
- Minimize processed foods, sugars, refined flour, saturated fats, and alcohol
- Reduce caffeine intake
- Be aware of potential food sensitivities including gluten, dairy, or alpha-gal meat allergy
Environmental Health
- Investigate your living environment if you suspect mold, dust, or other allergens that may worsen symptoms
Mental and Emotional Well-being
- Build strong support systems with friends, family, and community
- Consider professional counseling if needed
- Practice regular mindfulness meditation, restorative yoga, or spiritual activities
- Engage in activities that promote joy, positive thinking, self-compassion, and hope
Complementary Support
- Vitamins and supplements (discuss with your healthcare provider)
- Integrative or complementary practitioner support if needed
These lifestyle modifications should complement, not replace, medical care. Discuss any new interventions with your healthcare team to ensure they are appropriate for your individual situation.
Late Lyme Arthritis
Late Lyme arthritis is a late-stage manifestation of untreated or inadequately treated Lyme disease, characterized by significant joint swelling, pain, and inflammation, particularly in the knees.
Prognosis
Following appropriate antibiotic therapy, approximately 90% of patients with late Lyme arthritis recover fully from joint swelling, arthritis, and pain.
Antibiotic-Refractory Late Lyme Arthritis
Approximately 10% of late Lyme arthritis patients remain symptomatic despite extensive antibiotic treatment, a condition termed antibiotic-refractory late Lyme arthritis. Research has shown that live bacteria can no longer be found in the tissue or fluid of these patients. However, recent research shows that peptidoglycans, fragments from parts of Borrelia burgdorferi‘s cell wall, can persist in patients’ joints and trigger ongoing immune reactions that perpetuate inflammation. This understanding is driving the development of improved diagnostic tests and novel treatments for antibiotic-refractory late Lyme arthritis.
