Learn about Dysautonomia and POTS from Brit Adler, MD, Assistant Professor of Medicine, Division of Rheumatology, Johns Hopkins University School of Medicine.
Dr. Adler is a translational physician-scientist with an interest in postural orthostatic tachycardia syndrome (POTS) and dysautonomia that can occur in Lyme disease and COVID patients. She evaluates patients in the Johns Hopkins Autonomic Testing Lab.
What is Dysautonomia?
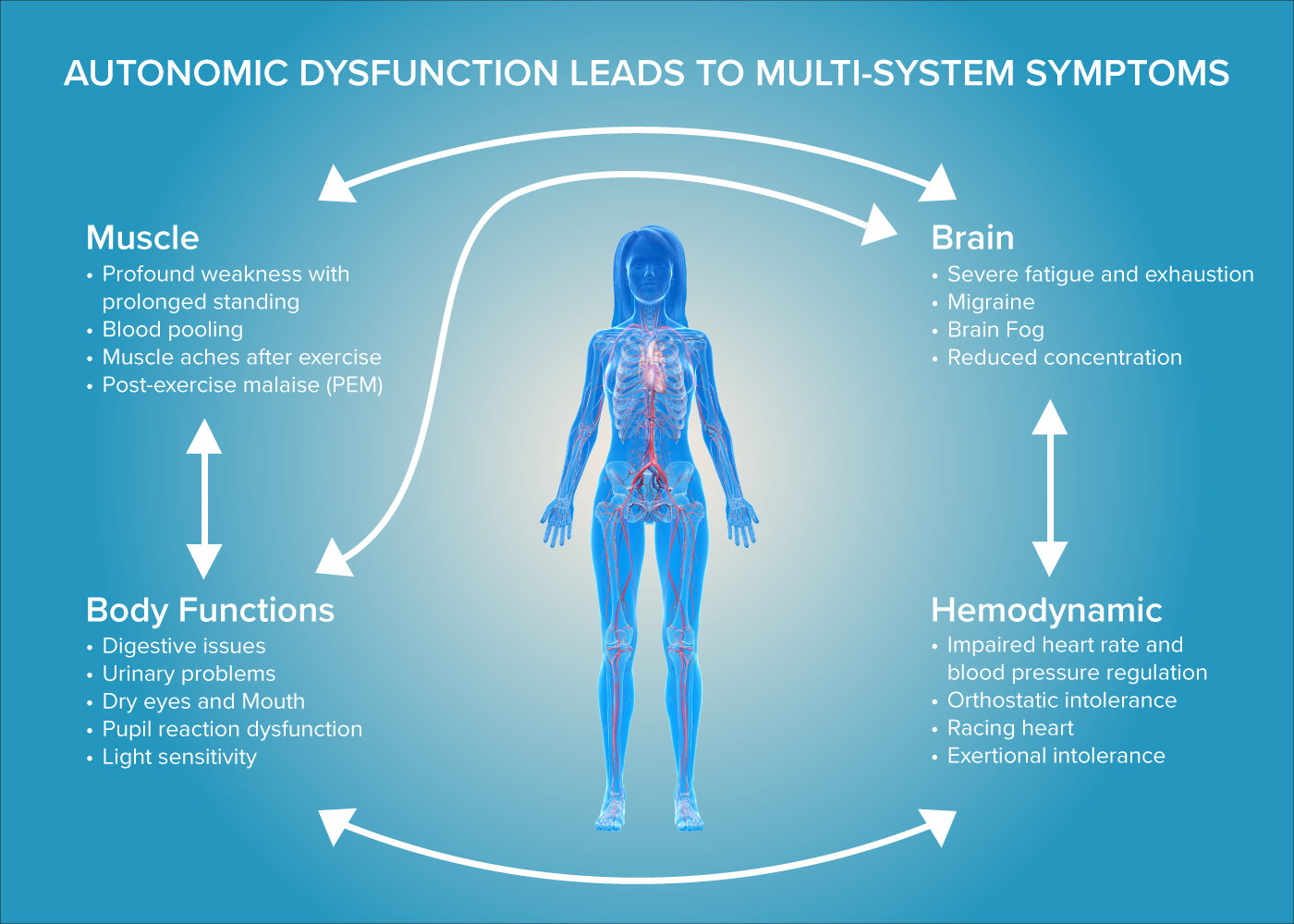
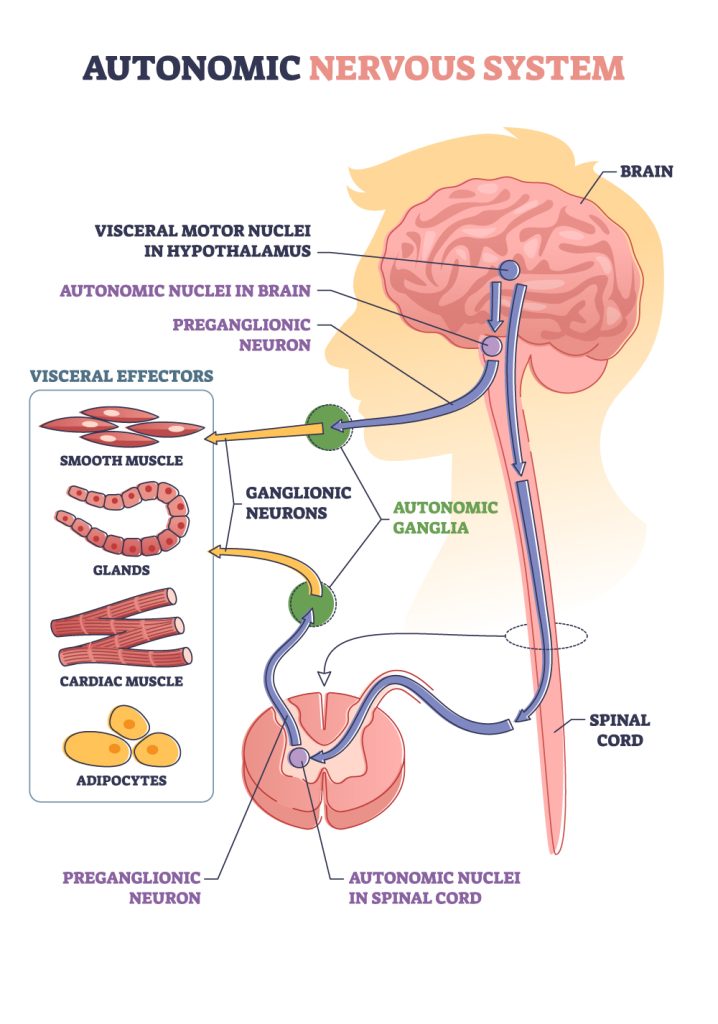
Dysautonomia is a disorder resulting from dysfunction of the autonomic nervous system, which is a major component of the peripheral nervous system. The autonomic nervous system regulates involuntary body functions, such as heart rate, blood pressure, breathing, digestion, body temperature, sweating, and tear production.
What is POTS?
POTS (postural orthostatic tachycardia syndrome) is a common manifestation of dysautonomia.
POTS occurs when the body’s autonomic nervous system fails to properly control heart rate and blood pressure regulation upon standing, leading to orthostatic intolerance or trouble standing up without feeling sick or lightheaded.
Can an infection trigger POTS?
Yes! Many infection-associated chronic illnesses are associated with POTS, including Lyme disease, long COVID, ME/CFS, and MS. However, infections are not the only cause of POTS.
POTS Symptoms can be debilitating and include:
- Brain fog
- Severe fatigue and exhaustion
- Profound weakness with prolonged standing
- Racing heart
- Exertional intolerance
- Muscle aches
- Lightheadedness
Incidence of POTS
POTS was estimated to affect between 500,000 and 3 million people in the US before the COVID-19 pandemic. The incidence rate of POTS has increased substantially from COVID-19, so these numbers have been growing.
Potential Risk Factors for POTS
- Exposure to infections, such as borrelia burgdorferi, COVID-19, Epstein Barr Virus
- Genetic and autoimmune susceptibility
- POTS disproportionately affects young women
- Hypermobility or Ehlers Danlos Syndrome (EDS)
What testing is available to clinicians to diagnose POTS?
Tests for POTS
- 10 Minute Stand Test
- Done in a doctor’s office to measure blood pressure and heart rate while standing for 10 minutes
- Heart rate increase of more than 30 beats per minutes with standing is diagnostic of POTS
- Tilt table test
- A more complicated test that includes continuous monitoring of heart rate and blood pressure while lying down and while suspended in an upright position on a tilt table
Tests for other aspects of Dysautonomia
- Motility testing for gastrointestinal dysautonomia
- Determines what area of the gut is affected
- Quantitative sudomotor axon reflex test (QSART)
- Measures the nerves that control sweating
- Skin biopsy to detect small fiber neuropathy, which is commonly present in patients with dysautonomia
- Detects decrease in density of the small nerve fibers in the skin
In the future, the Johns Hopkins Autonomic Testing Lab plans to offer:
- Transcranial Doppler Ultrasound
- Measures the change in blood flow to the brain with tilt
What are the limitations of current diagnostics?
Dysautonomia is a dynamic disease that can wax and wane, and diagnostic tests on a patient’s good day may not have positive findings despite the patient’s history of symptom flares.
Treatments for Dysautonomia
Beneficial lifestyle approaches
- Increased fluid and salt intake to optimize circulation and improve blood flow
- Compression stockings
- Abdominal binder to help pump blood back up to the heart and brain
- Patient-tailored exercise programs designed for patients with dysautonomia since exercise may not be well-tolerated
Medications
- Medications to improve gut motility
- Medications to improve circulation
- By reducing heart rate
- By increasing blood pressure
- Medications to target autonomic nervous system
- In clinical trials, immunomodulating medications such as IVIg (Intravenous Immunoglobulin) are being studied
- Antimicrobials for ongoing infections
Different infection-associated dysautonomia and POTS syndromes present with similar symptoms and may share common underlying pathologic mechanisms.
POTENTIAL MECHANISMS UNDERLYING INFECTION-ASSOCIATED DYSAUTONOMIA & POTS
The autonomic nerves or autonomic ganglia may be affected by:
- Chronic infection
- Autoimmune response triggered by an infection
- Damage to autonomic nerves by an infection
- Neuro-inflammation triggered by debris left-over after an acute infection is treated
CHRONIC ILLNESSES ASSOCIATED WITH POTS
- Post Treatment Lyme Disease
- Long COVID
- Myalgic Encephalomyelitis/Chronic Fatigue Syndrome or ME/CFS
- Sjogren’s Syndrome
- Systemic Lupus Erythematosus
- Hashimoto’s Thyroiditis
- Celiac Disease
- Diabetes
- MS
- Other Infection Associated Illnesses
RESEARCH NEWS
Review Article by Brit Adler, MD, in Frontiers in Neurology: Dysautonomia following Lyme disease: a key component of post-treatment Lyme disease syndrome?
Brit Adler, MD, at the 20th Annual Advances in the Diagnosis and Treatment of the Rheumatic Diseases symposium at Johns Hopkins School of Medicine discusses Dysautonomia and POTS: What the Rheumatologist Should Know
In February, 2025, Global Lyme Alliance (GLA) announced new research grants to address critical gaps in Lyme disease research. Brit Adler, MD, received a GLA grant to lead a study investigating the link between Lyme disease and postural orthostatic tachycardia syndrome (POTS). The study aims to uncover prevalence, risk factors, and physiological changes in patients, potentially leading to improved treatment strategies and insights into the pathophysiology of the chronic manifestations of Lyme disease.
